Is Zimbabwe sliding towards obesity?
Roselyne Sachiti Features Editors —
An abundance of fatty foods, fizzy drinks and sugary treats as well as lack of exercise are the biggest contributors towards obesity. According to the latest Zimbabwe Demographic Health Survey (2015), 35 percent of Zimbabwean women between 15 and 49 years are obese while 12 percent of men have the same condition.
The report further states that overweightness or obesity is most common among women with more than secondary education (57 percent) and those from wealthiest households (50 percent).
Women in urban areas are more likely to be overweight than their rural counterparts (46 percent vs 28 percent). The same patterns are observed among men, according to the report findings.
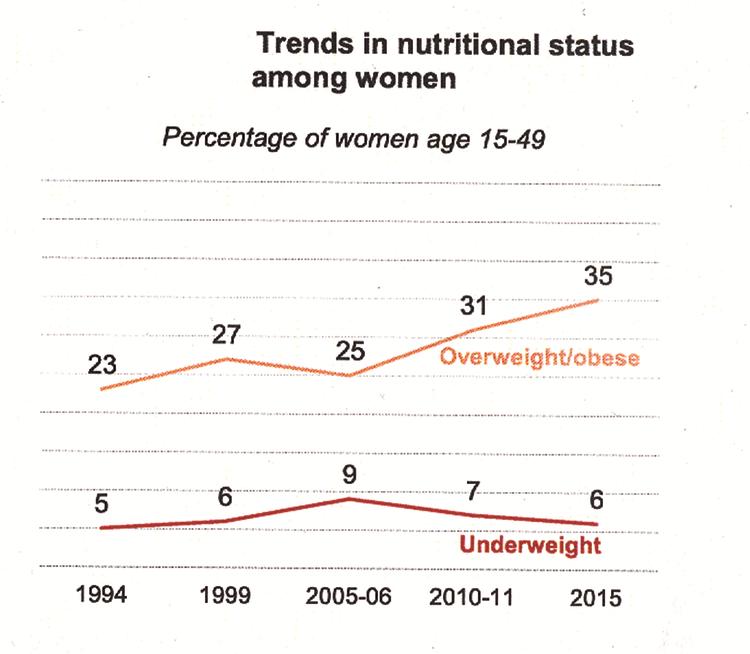
The report also says obesity among women has been on the rise since 2005-6, but remains essentially unchanged among men.
The margin for women who are thin (indicative of under nutrition) has remained fairly constant over the past two decades, peaking at 9 percent in 2005-6. In contrast, the proportion of women who are overweight or obese (indicative of over-nutrition) has gradually increased from 23 percent in 1994 to 35 percent in 2015.
Matabeleland South and North have the highest proportion of thin women (12 and 11 percent) respectively.
Director of Family Health in the Ministry of Health and Child Care, Dr Bernard Madzima says the current environment, which encourages energy intake and discourages energy expenditure, labelled as obesogenic, may be contributing towards the rise of obesity in Zimbabwe.
He said along with behaviour, unhealthy foods are believed to account for the increased prevalence of obesity.
“There is no one cause for obesity, but poor diet and inactivity appear to be leading factors. Genetic, physiological, metabolic, biochemical, and psychological factors can also contribute to it but to a lesser extent.
“Energy imbalance is a significant cause of overweight and obesity. People tend to eat more than they need resulting in energy intake exceeding energy expenditure.
“Excess weight can also accumulate during and after middle age because people reduce their level of activity and metabolism slows with age. Consequently, weight accumulates unless calorie intake is reduced,” he said.
Dr Madzima pointed out that factors that may be contributing to this obesogenic environment include an abundance of readily accessible, low-cost, palatable, energy rich foods, increasing consumption of soft drinks and snacks and an increase in the consumption of take away foods such as fried chicken, fried chips, fried sausages.
He also said the increasing portion size of restaurant meals, a decrease in energy expenditure (exercise, manual work) related to labour-saving devices such as remote control devices, motor vehicles, lifts also contributed immensely to obesity.
Dr Madzima added that an increase in sedentary leisure activities, such as watching television, playing video games, and sitting in front of a computer were also big contributors.
“Television watching may promote obesity by leaving less time for physical activity, lowering resting metabolic rate, and/or promoting greater meal frequency and food intake,” he said.
Why should we be concerned about obesity?
Dr Madzima says Zimbabweans should be concerned about being overweight as this leads to adverse metabolic effects on blood pressure, cholesterol, triglycerides and insulin resistance.
“Risks of coronary heart disease, ischaemic stroke and type 2 diabetes mellitus increase steadily with increasing body mass index (BMI), a measure of weight relative to height.
“Overweight is defined as BMI = 25 kg/m2. Obesity is defined as body mass index BMI =30 kg/m2,” he said.
He added that raised BMI also increases the risk of cancer of the breast, colon/rectum, endometrium, kidney, oesophagus and pancreas.
Obesity, according to Dr Madzima, increases the risk of complications during and after surgery and the risk of complications during pregnancy, labour, and delivery and causes psychosocial problems.
“Mortality rates increase with increasing degrees of overweight, as measured by BMI. To achieve optimal health, the median BMI for adult populations should be in the range of 21 to 23kg/ kg/m2, while the goal for individuals should be to maintain a BMI in the range 18,5 to 24,9kg/ kg/m2. There is increased risk of co-morbidities for BMIs in the range of 25,0 to 29,9 kg/ kg/m2, and moderate to severe risk of co-morbidities for a BMI greater than 30kg/ kg/m2,” he explained.
Dr Madzima said treatment of overweight and obesity involves appropriate nutrition assessment and dietary counselling by nutritionists and dietitians. The treatment based on the outcome of the assessment includes behaviour modification and exercise.
“If a significant cause of overweight is overeating, the solution is to reduce portion size and caloric intake. This is seldom easy. To accomplish it, one must undertake a weight reduction (low-calorie) diet. For the diet to be effective, one must have a genuine desire to lose weight.
“Behaviour modification involves changing eating and exercise behaviours thought to contribute to obesity and closely monitoring those behaviours. The fundamental behaviour modifications for a weight loss program are the development of a new and healthy eating plan and an exercise program that can be used over the long term.
“These are both major lifestyle changes, and one may need to participate in a support group or undergo psychological counselling in order to successfully adapt to these changes,” he emphasised.
Dr Madzima pointed out why it is important for people to learn the difference between hunger and appetite.
“Hunger is the physiological need for food that is felt four to six hours after eating a full meal. Appetite is a learned psychological reaction to food caused by pleasant memories of eating it. For example, after eating a full meal, one is unlikely to be hungry,” he said.
Physical activity
Increasing activity during weight loss helps preserve or increase lean body mass, which favourably impacts metabolic rate.
“With or without weight loss, increasing activity lowers blood pressure and triglycerides, increases HDL cholesterol, and improves glucose tolerance and cardio respiratory fitness,” he said.
He added that other types of obesity treatment are weight loss medication and surgical treatment.
“Weight loss medicines can be administered in conjunction with lifestyle changes of diet, behaviour modification and physical activity for people with a BMI of 30 or greater or for people with a BMI of 27 or greater with comorbid conditions, such as hypertension, type 2 diabetes, or dyslipidemia in some countries.”
However, Dr Madzima said, Zimbabwe currently does not have guidelines for treatment of obesity using weight loss medication.
“Surgery can also be performed in patients with severe obesity (BMI of 40 or BMI of 35-39,9). For clients who have major comorbidities, however, this type of treatment is also not very common in Zimbabwe,” he explained.
Although this may need further study, most rural women generally conduct a lot of physical activity and consume less energy dense foods which are unrefined and low in fat and refined sugar than their urban counterparts.
“Rural women walk longer distances to fetch firewood and water; they also work in the fields for longer periods of time which contributes to their physical activity.
“Their diet comprises mostly of food from plant origins which generally is low in fat and simple sugars. A combination of diet low in energy and high physical activity is known to contribute to the reduction in unhealthy weight gain.
“In contrast, most urban women have less physical activity through light household chores such as washing, tending small gardens, and spend a greater part the day watching television if they are not employed.
“The employed either drive or use public transport to go work and walk shorter distances. They usually have lighter duties at work that do not expose them high energy expenditure. The foods consumed by most of the women in the urban compared to the rural is high in fats and refined sugars and low in dietary fibre (eg fried meat, fatty meats, eggs, soft drinks, white bread with a fat spread, refined meal, snacks high in fats,” he added
He said it is difficult to say why there is a higher prevalence of obese women compared to men since there has been no study in Zimbabwe to investigate this. However, he added, other studies elsewhere indicated that women who were nutritionally deprived as children are significantly more likely to be obese as adults, while men who were deprived as children face no significantly greater risk of obesity.
In addition, women of higher adult socioeconomic status (SES) are significantly more likely to be obese, which is not true for men. There has been no further explanation to this phenomenon.
Zimbabwe National Practitioners Association President Friday Chisanyo agrees that the reason most urban women are obese is because of the lifestyle choices that include poor diet.
“Foods like pumpkins, cucumbers, okra, dried vegetables, sweet potatoes, wild fruits, ground nuts, sorghum and rapoko among others mostly eaten in rural areas are highly nutritious. Usually no chemicals like fertilisers are used on these crops making them safer.
“Cooking oil is also not used in the preparation of most of these meals making them healthier. This is in sharp contrast with their urban counterparts who feast on fast and artificial foods almost every day,” he said.
Chisanyo added there is need to grow more small grains as this will result in lower costs for consumers.
“You find out that a 10kg bag of processed maize meal costs much less than a 2kg packet of mhunga. This pushes the nutritious foods away from consumers. With less small grains grown, business people treble the price,” he added.
He said some practitioners under their union were offering counselling to obese patients who visit them for other problems.


You Might Also Like
-
Today is our 44th anniversary of independence, the day Zimbabweans achieved freedom, and did so under an elected Government, the double achievement being important. The freedom meant we became the owners of our own destiny, that we would decide what sort of country we wanted and could build that nation, without others deciding what was […]


Agriculture Journal

Comments